|
Clinical Study
Bacterial profile of high vaginal swabs in patients with preterm prelabor rupture of membranes at the Queen Elizabeth Hospital, Barbados and implications for antibiotic management
1 MBBS, Senior House Officer, Department of Obstetrics and Gynecology, Queen Elizabeth Hospital, Barbados
2 MBBS, MRCOG, FACOG, Consultant Obstetrician and Gynecologist, Maternal and Fetal Medicine Specialist, Department of Obstetrics and Gynecology, Queen Elizabeth Hospital, Barbados
Address correspondence to:
Keturah Murray
Queen Elizabeth Hospital, Martindales Road, St Michael,
Barbados
Message to Corresponding Author
Article ID: 100042G06KM2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Murray K, Robinson NT. Bacterial profile of high vaginal swabs in patients with preterm prelabor rupture of membranes at the Queen Elizabeth Hospital, Barbados and implications for antibiotic management. Edorium J Gynecol Obstet 2025;9(2):1–6.ABSTRACT
Aims: The aim of this study was to identify the bacterial organisms found in patients with preterm prelabor rupture of membranes (PPROM) at Queen Elizabeth Hospital (QEH). Hypothesis: “Escherichia coli (E. coli) is the most commonly isolated bacterial organism from high vaginal swabs in patients with PPROM at the Queen Elizabeth Hospital.” Preterm prelabor rupture of membranes refers to membrane rupture before the onset of uterine contractions occurring before 37+0 weeks of gestation. Genital tract infection is an important risk factor of PPROM. Identification of organisms associated with PPROM allows for targeted antibiotic therapy.
Methods: A retrospective cohort analysis was done using data from January 2024–December 2024 (12 months), to characterize the microorganisms identified in the high vaginal swabs (HVS) done in women admitted to QEH with a diagnosis of PPROM. A total of 31 women were included in the study. Under aseptic conditions, sterile high vaginal swabs were taken from the posterior fornix of the vagina of each patient. Fisherbrand modified amies charcoal transport medium was used. Swabs were transported to the laboratory within 24 hours of collection and stored at incubation temperatures of 35–37 °C. The samples were cultured on blood agar, Sabouraud Dextrose Agar (SDA), MacConkey agar, and Thayer–Martin agar for microbial isolation. The presence of creamy to white colonies on SDA was used to identify yeast. Gray colonies on blood agar confirmed bacterial vaginosis associated Gardnerella vaginalis. Data were collected from the antenatal ward admissions books and results of HVS were obtained from Schuynet (a web-based laboratory information system used at QEH).
Results: Of the 31 women, the results of 29 samples were obtained. Culture growth was present in the high vaginal swabs of 13 women (44.82%; 95% CI: 28.4–62.5%). Three different types of pathogens were identified: yeast in 10 women 34.48% (95% CI: 19.9–52.7%), bacterial vaginosis in 3 women; 10.34% (95% CI: 3.58–26.4%) and Group B Streptococcus in 3 women; 10.34% (95% CI: 3.58–26.4%).
Conclusion: Identifying these bacterial patterns is essential for selecting effective antibiotics. These data lead to the question of whether PPROM patients are receiving correctly targeted antibiotic treatment.
Keywords: Culture, High vaginal swab, Preterm birth, PPROM
INTRODUCTION
Preterm prelabor rupture of membranes (PPROM) complicates 2–4% of all singleton and 7–20% of twin pregnancies [1]. It accounts for 30–40% of preterm births, the causes are multifaceted; however, cervicovaginal infection is the most significant [2]. The main goals of treatment are to optimize maternal and neonatal outcomes, prolonging pregnancy where applicable, reducing risk of sequelae such as chorioamnionitis and managing risks of preterm birth.
Due to the lack of local data on bacterial profiles in patients with PPROM, our institution relies heavily on international guidelines, which may not fully reflect the unique bacterial prevalence and resistance patterns in our population. This gap can lead to suboptimal antibiotic choices, increasing the risk of treatment failure and adverse outcomes. Local data help clinicians identify which bacterial organisms are most prevalent in the community, allowing for more targeted antibiotic therapies.
The aim of this study was to identify the bacterial organisms most commonly found in patients with PPROM at QEH. The hypothesis was that E. coli would be the most commonly isolated bacterial organism. By identifying prevalent organisms and their resistance patterns, the study could help refine treatment protocols, reduce inappropriate antibiotic use, and ultimately improve maternal and neonatal outcomes in our population.
MATERIALS AND METHODS
This was a retrospective cohort analysis, done at a tertiary care center in the Department of Obstetrics and Gynecology, Queen Elizabeth Hospital, Barbados. This study examined patients who were admitted between January and December of 2024 with a diagnosis of PPROM. Only patients with singleton pregnancies were included. Each antenatal ward at QEH maintains an admission book that records the date and admitting diagnosis of all patients. Upon review, PPROM patients were identified and the results of their HVS were obtained via Schuynet (a web-based laboratory information system used at QEH). After the culture report was obtained, data were entered using Microsoft Excel for Microsoft 365 MSO (Version 2501). All patient data were anonymized. A total of 31 patients were included.
RESULTS
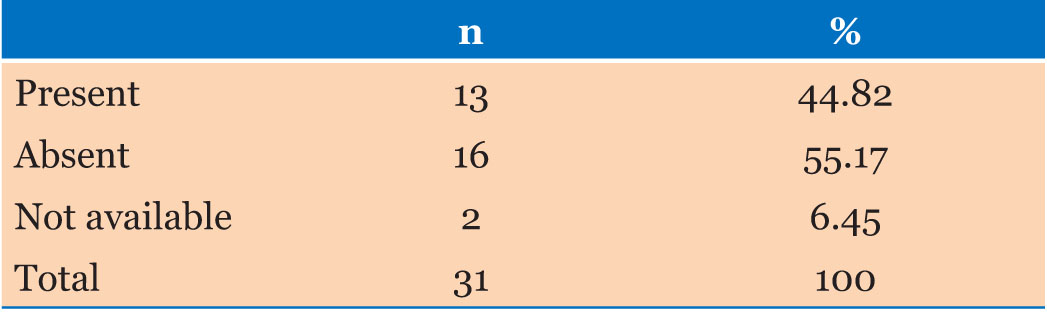
A total of 31 women with a diagnosis of PPROM were included in this study. Growth of organisms was identified in the high vaginal swabs of 13 women; 44.82% (95% CI: 28.4–62.5%), while no growth was reported in the remaining 16 women; 55.17% (95% CI 37.5–71.6%). Results were not available for two of the participants (6.45%) (Table 1).
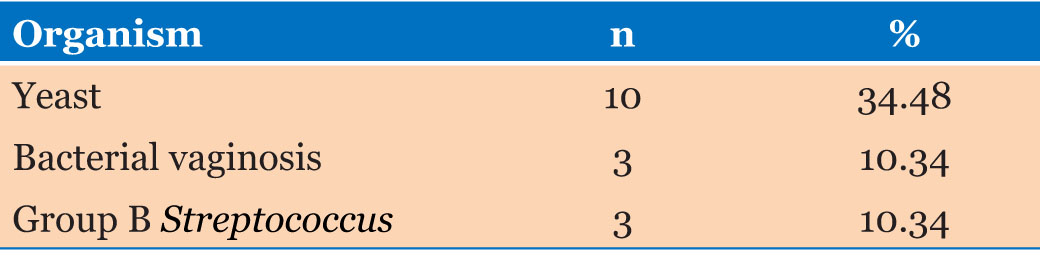
The HVS cultures from the samples collected identified 3 different types of pathogens. The organisms detected were yeast in 10 women; 34.48% (95% CI: 19.9–52.7%), bacterial vaginosis in 3 women; 10.34% (95% CI: 3.58– 26.4%) and Group B Streptococcus in 3 women; 10.34% (95% CI: 3.58–26.4%) (Table 2).
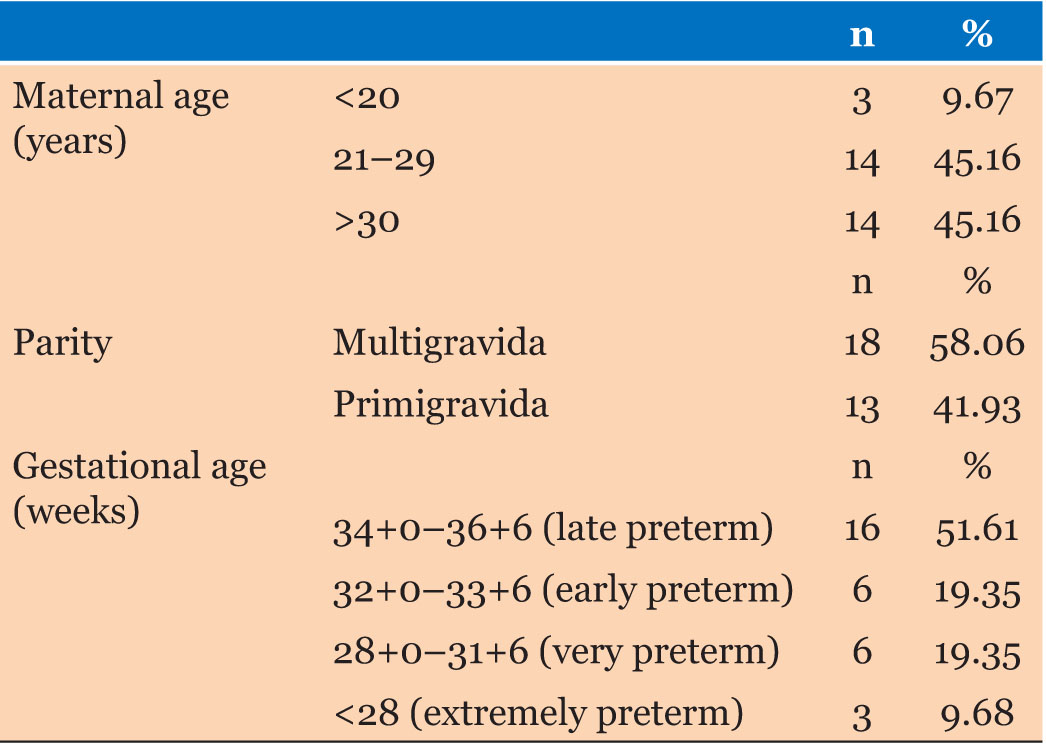
The participants in this study included women between 18 and 42 years of age with the mean age being 28.3 ± 6.2 years. The majority of persons were multigravida 58.06% (95% CI 40.8–73.6%), and most women 51.61% (95% CI: 34.8–68%) were admitted at late preterm gestation. Early preterm and very preterm admissions each accounted for 19.35% of women (95% CI; 9.19–36.3%) whilst 9.68% (95% CI: 3.35–24.9%) were extremely preterm admissions (Table 3).
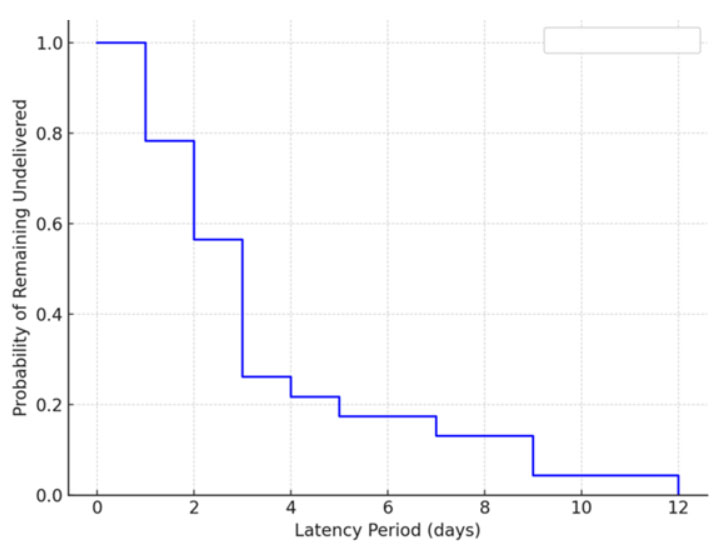
The mean latency periods were 3.1 (SD 2.5), 3.3 (SD 1.0), 2.3 (SD 0.5), and 6.7 (SD 1.2) days for late preterm, early preterm, very preterm, and extremely preterm groups respectively (Figure 1). A Kruskal–Wallis test demonstrated a statistically significant difference in latency periods across the groups (p = 0.046). The 95% confidence intervals were calculated using the Wilson score method.
DISCUSSION
In 2024, 1744 singleton births were registered at the QEH. Of these, 31 women were diagnosed with PPROM, representing 1.78% of pregnancies. This rate aligns with the established estimate that approximately 2–4% of pregnancies are complicated by PPROM.
Preterm prelabor rupture of membranes is a widely recognized condition that increases the risk of giving birth prematurely. The burden of PPROM ranges from maternal and neonatal mortality and morbidity to countrywide economic loss due to drug expense, hospitalization, absenteeism from the work, and expense to the health professionals [3]. It is responsible for around 30–40% of all cases of preterm deliveries. As PPROM is strongly associated with ascending vaginal infection, prophylactic antibiotics are widely used [4]. In this study, the vaginal bacteriological pattern of the women affected with PPROM was examined.
A total of 31 women were admitted to the obstetric wards with a diagnosis of PPROM. Most women 51.61% (95% CI: 34.8–68%) were admitted at late preterm gestation, 19.35% (95% CI; 9.19–36.3%) each were early preterm and very preterm, and 9.68% (95% CI: 3.35–24.9%) extremely preterm. This finding was similar to a cross-sectional study by Addisu et al., which looked at the prevalence of PPROM and its associated factors at a hospital in Ethiopia. In their study, 69.6% of women belonged to the gestational age of 34–36+6 weeks gestation [3]. Singh et al. also found the majority of their patients (47%) were admitted in this gestational category in their India based study [5].
In their analysis, 55% of the swabs were culture negative and 45% were culture positive. The positive culture rates in PPROM range from 21% and 45% [6]. The findings obtained in our study also fall in this range. Preetha found rates of 30% in their study [7] while Beevi et al. observed rates of 20% [8].
Among those cultures found positive, the organisms isolated were yeast (34.48%; 95% CI: 19.9–52.7%), bacterial vaginosis (10.34%; 95% CI: 3.58–26.4%) and Group B Streptococcus (10.34%; 95% CI: 3.58–26.4%). While these data reflect the small population studied in this local cohort, other studies demonstrate the fact that types of organisms and their frequencies vary widely. Beevi et al. observed different organisms; Escherichia coli (8.6%), Klebsiella (4.8%), Staphylococcus aureus (3.8%), Candida (1.9%) and Methicillin-resistant Staphylococcus aureus (1%) [8]. Naseha et al. [7], Svavya et al. [6], and Abdel-Hakeem [9] all also identified E. coli as the most common organism. Bargaje et al. however found lower rates of E. coli (1.67%) and higher rates of other organisms; Coagulase-negative staphylococci (13.33%) followed by Candida species (8.33%) and Klebsiella species (5%) among total studied patients [10].
The mean latency periods amongst the groups were 3.1–6.7 days. In a study by Singh et al., most women in their study (74%) delivered within 24 hours of PPROM. Only 11% had a latent phase of more than three days, and 28.5% delivered within 25–72 hours. In a study by Sultana and Karmokar, the mean latency period was 27 hours [11].
Some studies have demonstrated an inverse relationship between gestational age and latency period [12]. Dale et al. found that pregnancies with gestational age less than 26 weeks had a three-fold longer duration of latency period than pregnancies with gestational age of 32–34 weeks [13]. Similarly, the patients of extreme preterm gestation had latency rates of two times longer than early preterm patients. Overall, however, the results of this study did not reflect a directly inverse relationship. The average latency periods were 3.1, 3.3, 2.3, and 6.7 days for late preterm, early preterm, very preterm, and extremely preterm respectively.
A significant limitation to this study is that antibiotic sensitivity testing is not performed at our laboratory, even when cultures yield positive results. This research has brought to the forefront a key area of improvement, establishing protocols for sensitivity testing for all positive cultures. The incorporation of both antibiograms and rapid molecular diagnostics would play a key role in enhancing the detection and characterization of vaginal pathogens. While traditional culture methods provide valuable information, they may miss fastidious organisms or take several days to yield results. By integrating antibiograms, we can assess the antimicrobial susceptibility patterns of isolates of the common organisms which were identified in this study. Additionally, the use of rapid molecular diagnostics, such as polymerase chain reaction (PCR) assays, would enable the direct detection of key bacterial species and resistance genes from high vaginal swabs. This approach offers faster turnaround times and higher sensitivity. Together, these strategies would provide a more comprehensive and timely understanding of the vaginal microbiota and its resistance patterns, ultimately improving patient management and antibiotic stewardship.
The relatively small sample size may not be sufficient to capture the full spectrum of bacterial patterns associated with PPROM. However, in resource-limited settings, large-scale prospective studies are not always feasible. The strength of this small retrospective cohort therefore is that it sheds light into the microbiological profile of high vaginal swabs in patients with PPROM.
Of note, the most common bacteria isolated was Group B Streptococcus. This study is the first of its kind in Barbados, as there is currently no local data available. While E. coli was initially anticipated to be the predominant organism based on findings from international literature, regional data suggest otherwise. A study conducted in Jamaica examining the microbiological profile of high vaginal swabs at a tertiary level hospital, found fungi to be the most commonly identified organism overall (headed by Candida albicans). A predominance of Group B Streptococcus (GBS) was found in the obstetric population. The findings of the present study are therefore consistent with regional patterns, reinforcing the importance of generating local data to guide clinical practice and antibiotic management [14].
Vulvovaginal yeast infections in pregnancy are common and can cause extensive inflammation. Pregnancy-associated changes such as increased estrogen levels, glycogen-rich vaginal secretions, and reduced vaginal pH contribute to this phenomenon [15]. The presence of yeast identified on a HVS can represent colonization, infection, or contamination. In asymptomatic patients, this is more likely to represent colonization. In the context of PPROM colonization can potentially carry greater clinical significance. Neither Gigi et al. nor Schuster et al., however, were able to identify evidence of strong statistical significance of adverse pregnancy outcomes associated with yeast infections [16],[17]. While contamination from the vulva or perineum during sample collection is possible, consistent and high rates of yeast isolation across samples would support colonization as a more likely explanation.
Vertical transmission of Candida can occur as a result of contamination of neonates when mothers with vaginal Candida colonization give birth [18]. Filippidi et al. found that although overall vertical transmission rates were low, the vast majority of colonized neonates were born to mothers vaginally colonized with a large quantity of C. albicans colonies (3+ or 4+), suggesting a correlation between candidal colony counts in the vagina of mother and Candida colonization in the neonate [19].
The optimal antibiotic regimen is unclear because multiple regimens have demonstrated benefit [20]. Our hospital has traditionally uses the Royal College of Obstetricians and Gynaecologists (RCOG) recommendation of erythromycin as first line treatment for patients with PPROM. The findings of this study underscore the need for antibiotic susceptibility testing to guide objective, evidence-based decisions about potential modifications to clinical protocols within our institution.
CONCLUSION
Maternal genital tract infection is one of the causes of preterm labor and PPROM. Most women in Barbados receive care at the QEH, rather than private facilities, therefore this research provides valuable insight into the local pathogenic profile of our population. The difference in findings between the local and international reports underscore the importance of research into local data.
REFERENCES
1.
The PPROM Foundation - PPROM Facts. [Available at: https://www.aapprom.org/community/ppromfacts]

2.
Sharma J, Tiwari S, Thapa D, Yadav R. Vaginal microflora in high vaginal swab in prelabour rupture of membrane: A descriptive cross-sectional study. JNMA J Nepal Med Assoc 2024;62(276):532–5. [CrossRef]
[Pubmed]
3.
Addisu D, Melkie A, Biru S. Prevalence of preterm premature rupture of membrane and its associated factors among pregnant women admitted in Debre Tabor General Hospital, North West Ethiopia: Institutional-based cross-sectional study. Obstet Gynecol Int 2020;2020:4034680. [CrossRef]
[Pubmed]
4.
Brown RG, Marchesi JR, Lee YS, Smith A, Lehne B, Kindinger LM, et al. Vaginal dysbiosis increases risk of preterm fetal membrane rupture, neonatal sepsis and is exacerbated by erythromycin. BMC Med 2018;16(1):9. [CrossRef]
[Pubmed]
5.
Singh N, Pattnaik L, Panda SR, Jena P, Panda J. Fetomaternal outcomes in women affected with preterm premature rupture of membranes: An observational study from a tertiary care center in Eastern India. Cureus 2022;14(5):e25533. [CrossRef]
[Pubmed]
6.
Ghose S, Sravya M, Yogamoorthi V. Vaginal bacteriological pattern in women with and without preterm prelabor rupture of membranes: A comparative study. J South Asian Fed Obstet Gynaecol 2023;15(5):526–9.
7.
Preetha N, Laviniya N. A study on the relationship between high vaginal swab culture and fetomaternal outcome in prelabour rupture of membranes at term. International Journal of Science and Research (IJSR) 2023;12(1):795–7.
8.
Amina Beevi P, Girija Kumari AG, Sudhamani C. High vaginal swab study in preterm labour and preterm premature rupture of membranes and its relationship with neonatal sepsis. J Evid Based Med Healthc 2018;5(30):2249–54.
9.
Abdel-Hakeem AK, Shawky HED, Mohamed AM, Mohamed KG, Elbadawy AA. Prevalence of microorganisms associated with preterm premature rupture of membranes in Mnia University Hospital. prospective study. Minia J Med Res 2024;35(1):80–5.
10.
Bargaje GM, Hussain R. Study of prevalence of genital tract infection in preterm labour and preterm premature rupture of the membranes following fetomaternal outcomes. Int J Reprod Contracept Obstet Gynecol 2024;13(12):3642–7.
11.
Sultana F, Karmokar A. A study on maternal and fetal outcomes of preterm premature rupture of membrane in Tertiary Medical College Bangladesh. J Med Sci Clin Res 2019;7(2):184–92.
12.
Colucci C, Barsanti F, Morucchio A, Lippi C, Baldassari B, Di Tommaso M, et al. Latency from premature preterm rupture of membranes to delivery and correlation with gestational age. Ital J Gynaecol Obstet 2023;35(Suppl No. 1). [CrossRef]
13.
Dale PO, Tanbo T, Bendvold E, Moe N. Duration of the latency period in preterm premature rupture of the membranes. Maternal and neonatal consequences of expectant management. Eur J Obstet Gynecol Reprod Biol 1989;30(3):257–62. [CrossRef]
[Pubmed]
14.
Reynolds G, Campbell L, Heslop O. Microbiological profile of high vaginal swabs collected over two years at a tertiary level hospital in Jamaica. International Journal of Infectious Diseases 2018;73S:3–208. [CrossRef]
15.
Soong D, Einarson A. Vaginal yeast infections during pregnancy. Can Fam Physician 2009;55(3):255–6.
[Pubmed]
16.
Schuster HJ, de Jonghe BA, Limpens J, Budding AE, Painter RC. Asymptomatic vaginal Candida colonization and adverse pregnancy outcomes including preterm birth: A systematic review and meta-analysis. Am J Obstet Gynecol MFM 2020;2(3):100163. [CrossRef]
[Pubmed]
17.
Gigi RMS, Buitrago-Garcia D, Taghavi K, Dunaiski CM, van de Wijgert JHHM, Peters RPH, et al. Vulvovaginal yeast infections during pregnancy and perinatal outcomes: Systematic review and meta-analysis. BMC Womens Health 2023;23(1):116. [CrossRef]
[Pubmed]
18.
Gedefie A, Shimeles G, Motbainor, H, Kassanew B, Genet C. Vaginal colonization and vertical transmission of Candida species: Prevalence and associated factors among pregnant women and their neonates at public health facilities of Northeast Ethiopia. BMC Pregnancy Childbirth 2025;25:22. [CrossRef]
19.
Filippidi A, Galanakis E, Maraki S, Galani I, Drogari-Apiranthitou M, Kalmanti M, et al. The effect of maternal flora on Candida colonisation in the neonate. Mycoses 2014;57(1):43–8. [CrossRef]
[Pubmed]
20.
Prelabor rupture of membranes: ACOG practice bulletin, number 217. Obstet Gynecol 2020;135(3):e80–97. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions Guaranter of Submission
The corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Keturah Murray et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.